


Williams Syndrome, "Syndromic Autism", and the Death of the Diametric Model
maybe the hyper-extroverts weren't autistic after all

Prior to the 1990s, identifying the cause of most genetic disorders was a difficult task. Large modifications to a chromosome — an entire extra or missing copy, or a huge chunk deleted or duplicated, or part of a chromosome grafted onto another entirely — were identifiable, but clearly comprised a small minority of all syndromes. Emerging technology that decade allowed for the discovery of ‘microdeletions’ and ‘microduplications’, missing or added regions too small to be seen on a traditional karyotype. Today we call these copy number variations; in aggregate they are surprisingly common, and most didn’t form a syndrome so distinctive as to be clinically discovered before the microarray era. But some did.
Williams syndrome, caused by a microdeletion on chromosome 7, affects around 1 in 7,500 people. It has a few known medical consequences, certain otherwise-uncommon cardiac defects, very distinctive facial features that to some observers feel “elfin” or “fey”. It is nominally associated with IQs in the mild intellectual disability range, but this masks intense variance; people with WS have almost no capability for spatial reasoning/“shape rotation”, with adults regularly incapable of performing spatial tasks neurotypical toddlers find easy, but vocabularies are way above those of any group with “real” IQs in the same range. None of this, by itself, is what made WS famous.
People with Williams syndrome are exceptionally extroverted, absolutely fascinated by people, and have no concept of distrust. The term “overfriendliness” gets thrown around, which on the one hand is very “when you see people through a disordered lens, everything they do is a disorder”, and on the other hand is flatly true at the “enthusiastically gets into the Free Candy van” extremes. This is apparent from early childhood; infants with WS are way more interested in their parents than other infants, who already like staring at their mothers at any opportunity. In the second ever description of the syndrome, by a cardiologist far more interested in its heart defects than its other consequences, it was nonetheless so prominent for him to note that “[a]ll have the same kind of friendly nature—they love everyone, are loved by everyone, and are very charming” (Beuren et al., 1962, p. 1235).
In particular, people (especially children) with WS don’t seem to have a concept of “strangers”. Most infants and toddlers are anxious around new people, and shirk back if left alone in a room with a stranger; infants and toddlers with WS enthusiastically engage with playmates and doctors they’ve never seen before in their life. They totally shatter the curve on “how much of that do kids do”; Mervis and Klein-Tasman’s (2000) description of studies assessing this is a long line of “all 25 control kids refused to look at the doctor, all 25 kids with WS spent the whole time looking at and engaging with the doctor”.
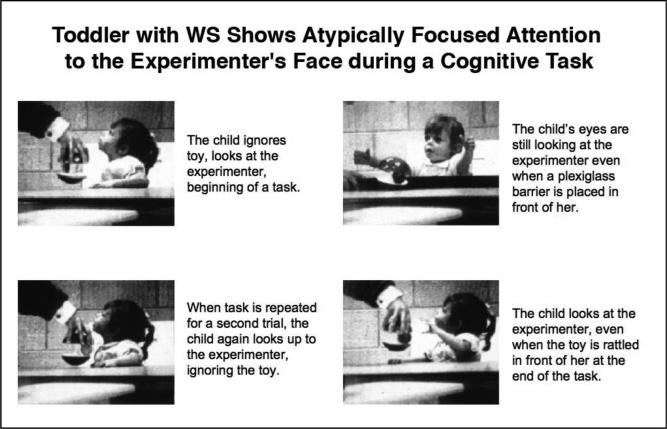
People with WS are remarkably fixated on faces. They make extreme eye contact. Children will overlook their favourite toy to focus on the person offering it. There’s something of a “staring into your soul” tendency, with Mervis et al. (2003) settling on “intense” as the best word for how an infant with WS looked at her playmates:

They have exceptionally strong affective empathy. Mervis gives an anecdote of a girl with WS at a party noticing a boy had stubbed his toe, and immediately running across the room to ask if he was okay. This sort of narrative is typical; “high empathy” keeps coming out as a distinctive WS trait in personality measures.
Given all of this, Williams syndrome is the famous, archetypal “anti-autism”. The behavioural phenotype is immediately and drastically unlike autism. Some evidence suggests opposite patterns on a neurological level, inasmuch as autism neuroscience is worth paying attention to (Fishman et al., 2011; Lew et al., 2020).
Around 10% of people with Williams syndrome are diagnosed with autism.
This is not quite as obviously insane as it sounds at first glance. It remains clearly wrong, but there’s a method to the madness.
There are genuinely traits of interest shared between autism and Williams syndrome. Beneath the obvious counterpoints, autism and WS overlap at just the points they “should” — they share many non-social traits, which are much more distinctive to autism than “idk it’s when you don’t have friends”. For one, they, uh, don’t have friends — okay, scratch that.
People with Williams syndrome have much poorer cognitive than affective empathy. They’re bad at “social cognition” — at understanding the correct thing to do in a social situation, or picking up on subtle hints. I’m not sold that this should be considered a disproportionate impairment for mildly intellectually disabled people, but okay, it does serve as a strong juxtaposition to the hyper-affection. Significant generalized anxiety is a big part of WS, affecting most people with the syndrome. Adults with WS tend to have few friends and be socially isolated (Jawaid et al., 2012), which, look, this is clearly for different reasons to why autistic people do, but…
All of this is the easily dismissed “there is obviously more than one reason to be bad at social skills” stuff. But there are real parallels! Most people with WS have stereotyped behaviours/“stimming”, and like for autistic people, this seems to emerge in part from sensory hypersensitivity (Riby et al., 2013). Virtually all of them have such hypersensitivity and unusual sensory processing, particularly around hearing (Glod et al., 2020). People with WS have very strong musical skills, ranging from just a ‘relative strength’ to being markedly better than most people (Thakur et al., 2018).
The extreme mismatch of cognitive skills in WS is also reminiscent of autism. While people with Williams syndrome are overall not-wrongly-described as intellectually disabled, the extreme spatial/vocab disconnect is like nothing else. People with Williams syndrome are incapable of the most basic figure-reproduction tasks, but play with words far better than children who test as similarly disabled:

Defenses of autism diagnosis in Williams syndrome tend to sound like this — “well, yes, they don’t come across as autistic at first, but when you look into it they do”. There’s some good scientific inquiry here, and I applaud it. Non-social autism traits are genuinely more core than social ones, and prioritizing them avoids a lot of overdiagnosis mistakes. In a sea of “probably all introverted disabled kids are autistic”, it’s a nice change to have “the extroverted disabled kids are autistic too, because they share the non-social traits”. It doesn’t become right, of course. It’s possible to overcorrect and look so hard at the non-social traits you ignore that the rest of the symptoms are “hyper-social, hyper-empathic, hyper-interested-in-people, hyper-looking-people-in-the-eyes”. If we want a concept of autism even vaguely recognizable to Kanner or Asperger, it should probably exclude Williams syndrome.
This originates out of the concept of “syndromic autism”. No one is quite sure what causes autism, aside from “not vaccines”. “Autistic traits” pop up in a broad variety of populations, some of which cluster with autistic people; the minimum line for diagnosis doesn’t quite carve reality at the joints.
Some people who are above 50th percentile autism also have a known genetic disorder, and in particular a known intellectual disability syndrome. ID, itself, is not a category that carves reality at the joints. It’s “people with an IQ below 70 and commensurately poor scores on adaptive functioning tests”; the largest share of people who end up in this classification are just “not very bright” people whose non-brightness seems serious enough to be worth labelling for disablity services. Mild ID (the 50-70 IQ range) blends in with the cognitive range of the general population, and many (most?) mildly ID people never receive a diagnosis.
Another large share of ID, though, and particularly of ID below the 50 IQ mark, is caused by known syndromes. Some of these have non-genetic causes (e.g. fetal alcohol syndrome), but most, and in particular most severe intellectual disability syndromes, are caused by genetic or chromosomal variations. Many intellectual disability syndromes have associated “behavioural phenotypes”, which are rarely as extreme as Williams or Lesch-Nyhan, but describe loose personality trends. Down syndrome is the most common and most famous intellectual disability syndrome; you might be familiar with stereotypes of people with Down’s as “happy” or “friendly”. Some of these behavioural phenotypes include autistic traits.
I think a large share of all current “severe autism” is diagnostic substitution — intellectual disability without uniquely autistic characteristics that has been labelled as autism due to the term’s greater recognizability. ID is still not a particularly well-known term, and its predecessor “mental retardation” became a slur like ten years before it was removed from the DSM. Many autistic traits are “developmentally normal” in severe ID, and the early conceptualizers of autism didn’t actually consider autism and severe ID a legitimate dual diagnosis. For “idiopathic” severe disabilities, where no one is quite sure what caused them, this is harder to demonstrate — but syndromic autism tends to show it real hard.
Williams syndrome is the canary in the coalmine for syndromic autism. It’s the line that marks that no matter how unlike autism a given intellectual disability syndrome is, people will look for autism in it. In intellectual disability syndromes that don’t have a famous extremely-not-autism profile, diagnosis rates soar several times higher (Richards et al., 2015). The more severe a disorder is, the higher “autism rates” tend to be. Within disorders, people diagnosed with autism tend to be the most severely affected; Down syndrome (despite its also-very-distinct behavioural phenotype) has about the same supposed ASD prevalence as WS, and this consistently tracks to “people dual diagnosed with Down’s and ASD have the most severe intellectual disabilities” (Hamner et al., 2019).

I am excruciatingly skeptical about stuff like “diagnosing autism in the 10% most impaired people with Down syndrome”. I don’t reject the existence of autism in genetic syndromes out of hand — quite a few seem genuinely associated with it — but the easiest ones to spot real autism in are the mild ones, where actual autistic traits are present without confounding by intellectual disability. Sex chromosome aneuploidies (extra or missing sex chromosomes) are a great example of this, and split in very interesting ways with complex implications for the ASD gender ratio. Some copy number variations pull this off, too.
As aforementioned, Williams syndrome is a copy number variation (CNV). This is an umbrella term for structural variants (deletions or duplications) in a chromosome that are too small to see on the tests that were available in the early era of syndromology, but were quickly detectable once we were able to test chromosomes with more sensitivity. Most CNVs are small, with little or no clear impact, and don’t form obvious clusters. A very few are serious enough that they were recognized syndromes for decades before anyone knew what caused them. Many more are somewhere in between, clearly disorders once you can look at them, but not so distinctive that they constituted a diagnosis before.
An interesting thing about CNVs is that they’re reciprocal. In any recurrent CNV (one where modifications of the exact same region are prevalent in the population and cause a consistent-ish syndrome), deletions and duplications are both theoretically possible. In some cases, reciprocal CNVs are well-characterized. In others, usually where the more common version is itself rare and poorly-understood, the reciprocal CNV exists on the level of a handful of disparate case studies.
This is exciting, because you get a real-world model for the effects of “opposite” genetic changes. Trends emerge. Losing genes seems to be more severe than gaining them. In some cases, particularly for physical traits or where the phenotype of one CNV is particularly striking, reciprocal CNVs form an “opposite” profile. In others, it’s more complicated.
Many CNVs are more common in people diagnosed with autism or schizophrenia, so a lot of people are interested in how this presents in reciprocal CNVs. One person particularly interested in this is Bernard Crespi.
I mentioned Crespi’s work in my last post. He’s a biologist whose work is primarily on social behaviour in insects. In the late 2000s, he teamed up with the sociologist Christopher Badcock to devise what has been called the diametric model or imprinted brain hypothesis — the idea that autism and schizotypy are opposites on the neurological, genetic, and evolutionary level. If you just ignore the huge and constant overlap between them, and the fact the original paper was filled with stuff like “the connection between schizophrenia and homosexuality” cited to a paper from 1962 about how schizophrenia from a psychoanalytic perspective is repressed homosexuality, and the part where the theory considers depression part of schizophrenia and thus incompatible with autism, it’s a great idea!
But Crespi is nonetheless a smart guy who drills down on things in a way most people in this field don’t. In particular, he’s like the only person who isn’t me and who really recognizes the implications of “schizotypy is a bigger part of the schizospec than schizophrenia is”. He and especially Badcock are good self-promoters, and Badcock’s interpretation of the model in particular (which, unfortunately, is a much worse interpretation) has gotten a lot of pop-psych currency.
Because Crespi is approaching this from a biologist’s perspective, he pays a lot of attention to CNVs. There’s a particular rhythm to his work that you’ve probably seen pop-psych presentations of (there was apparently a Wikipedian into it, because tons of our articles take it at face value):
CNVs have inherently “opposite” presentations, i.e. the complex phenotypes of a CNV (not the broad-strokes stuff like intellectual disability) must, by way of how gene dosage works, be opposite to one another
Some CNVs are more associated with autism diagnosis, while others are more associated with schizophrenia diagnosis
Reciprocal CNVs can differ on this, and certain patterns that correlate with autism or schizophrenia diagnosis in the general population (e.g. head circumference) imply these differences reflect real underlying opposites
Therefore, CNVs demonstrate that autism and schizophrenia are opposites
Point #3 manages to be less credulous about syndromic autism than most. Unfortunately, it’s still way too credulous. Williams syndrome tells us why.
The first reports of duplications of the WS region of chromosome 7 came out in the mid-2000s. Somerville et al. (2005) snagged the first known case. Back then, it wasn’t entirely clear what a “reciprocal CNV” should look like — no one with Williams syndrome seemed to have the duplication, so maybe it was lethal in utero, or maybe it didn’t do anything at all. Somerville found it an eight-year-old boy with an ADHD diagnosis and a mild intellectual disability, but speech delays far more severe than this alone could explain; he could barely speak at all, and communicated more with a mix of drawing and sign language.
As more reports came out, a portrait of the WS-dup syndrome formed. Like many duplications, it had a broad spectrum. About 25% of people inherited it from a parent, which is extremely rare in Williams syndrome. Some facial features were common, but not as consistent or distinctive as WS facies. It did pattern as the opposite of WS in some striking ways, with extreme speech delays and shyness. Berg et al. (2007), the first description of multiple children with the WS dup, remarked on the autistic traits many presented; even those who didn’t seem to be autistic per se had distinctive tendencies, like stimming or playing by lining up objects.
Crespi’s early work on the diametric model put a lot of stock into this. He broadly hypothesized that different CNVs caused “autistic spectrum” or “psychotic spectrum” conditions, where people with the former were unusually poor at mentalizing and people with the latter were unusually good at it. Crespi was (and is) critical of profligate syndromic autism diagnosis, arguing that disorders with a “shyness and severe anxiety” profile actually reflected hyper-mentalizing — that they were consequences of being too aware of others’ judgement.1 He also tried to track particular cognitive profiles to this distinction, arguing that autism was inherently linked to better spatial skills and schizophrenia to better verbal skills.2 WS and its duplication provided a fruitful avenue for this; people with WS were hypersociable, anxious, and had intense verbal-over-spatial skews, while people with the duplication seemed to be the opposite (Crespi et al., 2009).
A couple decades on, we have a solid idea of the “7q11.23 duplication” profile now. Severe speech delay remains a constant. Cognitive impairments are far milder than in WS, as is often the case in reciprocal CNVs; the median IQ is right at the bottom of the “average range”, and many people with the duplication are well above the population norm. Unlike WS, there’s no extreme strengths-weaknesses profile, but adaptive skills (generally “caring for yourself”) are much worse than raw intelligence. Autistic traits are very common, and maybe 20% are diagnosable; people without clinical autism per se often have subclinical traits, extreme clumsiness, social anxiety, and selective mutism. There are somewhat distinctive facial features (prominent forehead, flat eyebrows) and a tendency towards large heads, which is worth elaborating on.3 This is all alongside a handful of distinctive physical concerns (see Mervis et al., 2021 for a general overview of the syndrome).
Oh, and it’s a huge risk factor for schizophrenia.
Our knowledge of CNVs in particular developmental disorders tends to come from large study populations specifically designed to identify potential genetic variants corresponding to diagnosis. One particularly interesting one is the Simons Simplex Collection. It’s a genetic repository of a few thousand autistic people from “simplex” families — generally defined, immediate families where only one person is autistic, with allistic parents and siblings.
The Simons Simplex Collection isn’t interested in your lazy definitions. It requires families have no diagnosed autistic members out to third-degree relatives (cousins and equivalent). Parents and siblings (including half-siblings) can’t ever have been referred for an autism assessment, can’t have or “possibly” have an intellectual disability or severe learning disability (e.g. dyslexia), and can’t be schizophrenic. Siblings with literally any developmental or psychiatric attention in their entire lives are suspect, and screened rigorously for potential exclusion. Autistic participants can’t have been born prematurely and need to be “not so severely disabled as to make diagnosis obviously suspect”. Everyone in the immediate family gets subjected to a full battery of autism assessments to confirm diagnosis/non-diagnosis. It’s really impressive work — I suspect literally every really-autistic person in the United States from a bona fide strict-simplex family is in there.
And they still keep having to kick people out, because they turned out to be multiplex families the whole time! This is all you need to know about how hard autism runs in families.
Sanders et al. (2011), studying the Simons Simplex Collection, found the first hard suggestion that autism was more common in people with the WS duplication. Their numbers corresponded to about 1 in 1000 participants having the duplication, compared to what’s thought to be about 1 in 15,000 people in the general population. A lot of supposed “autism-causing CNVs” are sketchy — people with them have significantly lower IQs than matched “idiopathic” autistic people, say, or more generalized early delays,4 or way lower scores on distinctively autistic metrics like “stereotyped behaviours”. The duplication has a little of this, but mostly avoids it; people in the Simons Simplex Collection with the duplication had basically identical IQs to other participants and very similar overall autism profiles, aside from tending to be more irritable.
1 in 1000 is probably an overestimate for the general autistic population — “simplex autism” is more associated with CNVs, in part because it’s more diagnostically substituted — but the WS duplication doesn’t look like the classic diagnostic substitution syndromes. Hell, there’s one case of an autistic guy having four autistic kids and all five of them turning out to have the duplication (Earhart et al., 2017).5 It’s unlikely to be a massive overestimate. This gets you something maybe 10-15 times more common amongst autistic people than baseline.
Some CNVs are associated with schizophrenia. Compared to their associations with unusual early development, these associations are pretty weak (Kirov et al., 2013), and it’s disproportionately true for people with particularly low IQs (Lowther et al., 2017). There’s likely some Questionable Diagnosis here too — any forensic or low-income-community clinician can tell you “low-functioning” people end up with SZ diagnoses for all sorts of reasons. But inasmuch as CNVs alter development in “direction of an unusual neurotype” ways rather than “generalized impairment” ways, they should and appear to do so here as well.6
Mulle et al. (2014) found that the WS duplication was definitely a schizophrenia CNV. They first became suspicious when they noticed that in a group of 554 people diagnosed with schizophrenia, two unrelated individuals had a duplication of the same region. Expanding their search to 14,387 people described across multiple studies they were able to attain the data for, they found eleven had the WS duplication — well above the number you’d expect by chance.
For some of these carriers, the researchers were able to find out some details of their childhood. At least two were…autistic. Both members of the original 554 were extremely anxious and withdrawn children with restrictive eating disorders and severe obsessive-compulsive behaviours, who had delayed developmental milestones but graduated from college; one had recurrent “tics” from early childhood and was “suspected to have autism”. Not to put too fine a point on it, but, look, the paper itself says “social withdrawal”, and then you get into the supplementary material and it’s that. This is why psychiatry needs more phenomenology. The only other two with any childhood descriptions were withdrawn and/or disproportionately late talkers.
What have we found since then? Yeah, it seems to be a real association both ways. The aforementioned Kirov estimates about 6% of people with the WS duplication will be diagnosed with SZ; the way they calculated prevalence makes me suspect it’s an overestimate, but you can go a lot lower than that and still mark a real increase. Most people with the CNV are neither autistic nor schizophrenic, but the midpoint on the autism and schizotypal spectra seems to be further down than average. It’s one of the “real” CNVs — one where the effect seems to actually correspond to what people experience in the general population, rather than a diagnostic substitution nightmare.
This is plenty interesting from the “reciprocal CNVs as opposites” hypothesis. People with Williams syndrome are extremely not-autistic. They’re not especially susceptible to psychosis; there are only a few case studies, and some of those suggest an excruciatingly questionable diagnosis. Neuroanatomical and (inasmuch as that matters) functional patterns in the duplication are opposite to those in Williams syndrome and resemble those of autistic people (Prontera et al., 2014). If you want to be tongue-in-cheek, you can propose WS marks “extreme allism” — the most dysfunctional variant of the neurotype-space we carve out as NT, showing all the problems that emerge when exaggerated past what our society has built itself to accommodate. There are problems with this, of course. But if you want CNVs to be opposites, then WS as the pathological lack of what the duplication grants — unambiguously increased autism and schizotypy — checks out.
This isn’t what Crespi wants.
Crespi & Procyshyn (2017) is an about-face. The hypothesis was falsified. Here was a reciprocal CNV with the exact patterns Crespi predicted would flow out a certain way. One CNV caused smaller heads/smaller brain size; the reciprocal version caused larger heads/larger brain size. One CNV caused a hyper-developed vocabulary; the other caused speech delays. One CNV caused an extreme skew towards verbal abilities over spatial; the other didn’t cause any skew, but, eh, close enough. One caused a famously, notoriously hyper-sociable profile, yet mixed with a thick stew of anxiety, which matched what Crespi declared schizotypy to look like; the other caused…autism and schizophrenia.
The constant Crespian defense of the diametric model is “that isn’t autism, it’s schizotypy”. This gives away far too much — if schizotypy is something that is constantly identical to autism, it’s a little tricky to present them as “opposites”, and pointing this out is enough for most people to come around on the hypothesis being bullshit.7 It’s driven by a fundamental problem for the hypothesis — psychosis is (supposed to be) fairly “unmistakable”, so an unambiguous diagnosis of psychosis in someone autistic falsifies their incompatibility. Accordingly, any dual diagnosis must be labelled as misdiagnosed schizotypy, leading to a concept of schizotypy that apparently includes most ASDs.
Once the WS duplication became a schizophrenia CNV, Williams syndrome had to become autism. Crespi proclaims in his 2017 paper that WS reflects the “active but odd” subtype of ASD — the autistic extroverts who socially approach people, but have no idea how they work. This is a real group of autistic people, who have been recorded for as long as autism is a concept. They are not like people with Williams syndrome. There are no autistic toddlers who are that obsessed with faces. Autistic extroverts are their own interesting and understudied cluster, but can’t be rounded to “extroverts with bad social cognition”.
Crespi (2019) expands upon this, linking it back to the core of the “imprinted brain” claim. The basic idea underpinning the hypothesis since its beginning is that autism reflects “too much paternal influence”, and schizotypy “too much maternal influence”. A small handful of genes are imprinted, meaning one parent influences them more than the other. Paternal overinfluence, thus, would cause children to put more stress on the mother — having faster brain growth, being hyperactive, sleeping less, being more selfish. Maternal overinfluence would do the opposite. By 2019, CNVs like those in the Williams syndrome region had screwed this so hard that Crespi’s presentation looks little like autism or schizotypy at all:

Would Kanner or Asperger have thought of autistic children as “strongly attached”?
Even Crespi has to admit, in this paper, that Williams syndrome “exhibits a mixture of non-autistic traits” with autistic ones (Crespi, 2019, p. 3). Non-autistic traits like, I dunno, presenting the actual diametric opposite of everything the model describes as autistic. If you turn “autism” into “hyperactivity and attention-seeking”, you can fit Williams syndrome in there, but you don’t leave much room for autism.
There’s one more paper that leans right into this. It has, for our purposes, a conveniently provocative title: “The Paradox of Copy Number Variants in ASD and Schizophrenia: False Facts or False Hypotheses?” (Crespi, 2018). Here, he argues that the “opposing effects” hypothesis of reciprocal CNVs has to be true, given everything we know about their physical impacts. This is questionable — it’s clearly not true for VIQ-PIQ gaps, which are more objectively measurable than fuzzy arguments over whether someone is more autistic or more schizotypal — but even taking it at face value, it gives away too much.

You can’t present the opposite effects of CNVs on brain size as uncritically supporting a diametric model when WS duplications are right there! WS duplications clearly present an “autism-direction” change, if we even want to believe this change unambiguously exists — which is best described as “unclear”, given fn 3 and the iatrogenic effects of neuroleptic drugs on brain size.
Every single prediction of the diametric model says that WS duplications cause autism and, by extension, not schizophrenia. They cause both. Presented with this inconvenient fact, the model jumped to the opposite — that WS duplications are “really” schizophrenia, and thus Williams syndrome itself is “really” autism.
This fundamentally invalidates the whole affair. We found something that would falsify the model if it were true, it was true, and now it’s falsified. Its persistence despite this is not especially endearing. Outright taking the opposite position shows every crack in the model; its current version is unfalsifiable, and by extension pseudoscientific. And it means you have to call Williams syndrome autism.
No one is quite sure, these days, how best to understand autism. Everyone has their own theory, battling it out for acceptance, casting a long shadow over the moonless night of the real world. A good starting place might be “not Williams syndrome.” The fact we cannot agree on this starting place says little good.
This is best described as “disputable” — autistic people certainly seem socially anxious. I’m actually sympathetic to an argument that social anxiety is less common in autism than expected compared to general anxiety of which social anxiety is just an offshoot, but it’s one of those things that sounds like “depression is the opposite of autism” in terms of real-world sanity. I’m not entirely sure how the diametric model best conceptualizes the subset of autistic people who have one or both of those things chronically. The easy claim is “that’s still misdiagnosed negative schizotypy”, but this quickly runs you into a framework where all autism is misdiagnosed negative schizotypy. Anecdotally, if I’ve ever noticed a schizotypy-depressiveness correlation in autistic people, it’s slightly negative.
This is also best described as “disputable”, but it’s more complicated. Important introductory note: “nonverbal intelligence” and “spatial intelligence” are not synonyms. Spatial reasoning is a subset of nonverbal IQ, and probably the less important one. The other one tends to be called something like “fluid reasoning” or “nonverbal reasoning” and in theory is supposed to gesture in the direction of “pure problem-solving”, but whether it actually does this is questionably evidence-based. Historically, the WAIS/WISC had a dyadic “verbal IQ” and “performance IQ” structure; this distinction is not real anymore but still worth making for reasons, and many other IQ tests still do it.
IQ testing in schizophrenia is messy and awful, but evidence suggests a VIQ > PIQ profile is more common than it would be in the general population. Notably, any apparent negative correlation between schizophrenia PRS and IQ test performance seems to only be a PIQ thing (Hubbard et al., 2015; Mitchell et al., 2022). Nonetheless, it’s not an exceptionally strong tendency, and people have all sorts of profiles.
IQ testing in autism is even worse. The g concept (where all cognitive abilities are pretty well-correlated in NT populations) crashes and burns when exposed to autistic people. Donna Williams and Scott Aaronson both describe this well (putting aside whether Aaronson identifies as autistic, the particular profile he describes here is the most ludicrously autism-specific one conceivable, which does not occur in allistic children ever unless they have been locked in closets for 12 years with no exposure to the outside world). Autistic people have a tendency to get wildly incompatible scores on different tests, to get scores wildly incompatible with their obvious ability, to somehow floor and ceiling different scales, etc. It’s more common for this to present as disproportionately good nonverbal abilities, because “extreme speech/language delay without other developmental delays” is a traditional autism profile, but even within this framework it’s often only some nonverbal abilities. When the “Asperger’s versus high-functioning classical autism” distinction existed, higher VIQ in Asperger’s vs higher PIQ in HFA was a commonly-quoted part of it; this didn’t actually exist at first, but then people started diagnosing people with one or the other based on their cognitive profile, so later research found it. Science!
Autistic people tend to have large heads. It’s not an insurmountably strong tendency, but the median head circumference for autistic people is probably around the 60th-70th percentile in the general population, and macrocephaly (>97th percentile HC) is way more common than genpop. This is true across the whole spectrum, though some studies suggest biases one way or the other. In children, this is associated with unusually large brain size; it’s not clear if that’s still the case in adults, or if the growth curve slows at some point, but “big heads” stays the same.
Crespi conceptualizes autism as an overgrowth syndrome (i.e. head and body size are both large). This does not in fact appear to be true; autistic people have larger heads than predicted from body size. It’s true of a number of “syndromic autism” conditions, but THERE’S THE PROBLEM.
The jury is out on whether autistic people are born with big heads, or if there’s a period of unusually rapid head circumference growth in infancy. It’s probably both in different cases.
The diametric model claims schizophrenia is associated with smaller head circumference, so this produces an opposite between autism and schizophrenia. This is yet another thing best described as “disputable”. The usual study given to support this is a study of infant head circumference that is totally worthless (HC was rounded to the nearest whole centimetre, when 1cm differences are a huge deal in infant HC, and the difference after excluding premature babies is less than 1cm). As alluded, it’s not exactly clear that infant HC is increased in autism either. Studies of people actually diagnosed with schizophrenia suggest a tendency to larger HC (Bassett et al., 1996; Deutsch et al., 2013; Weinberger et al., 1987); Deutsch finds the strongest tendency, and that it also holds in first-degree relatives, implying this is true across the schizospec.
The most distinctive (note: this is not “universal”) pattern of autistic early development is one of disparities. Note the last paragraph of fn 2. It’s very common for autistic kids to, say, have extreme speech delays while walking at a normal or early age, or to read bizarrely early while not seeming particularly advanced in other developmental milestones, or to not smile responsively until they’re like 10, or otherwise ignore any baby book’s sense of “X milestone at Y age, which is a mandatory precursor to Z at A age”. Some writers consider motor delays a shibboleth for diagnostic substitution — their construct of autism excludes anyone who walked as late as they talked. “Syndromic autism” almost always fails this.
Case studies are weirder than anything you can come up with from first principles. The youngest child and only boy of the kids was XYY as well as having the WS duplication. XYY is a huge autism factor, and somehow he was probably the least autistic member of the family. This was seven years ago — I want a follow-up.
Schizotypy and autism have an interesting shared characteristic:
They are neurotypes, Types of Guy, whatever
The relatives of people diagnosed with a form of them, including a particularly unusual or dysfunctional form of them, tend to have the same thing themselves in lesser strength (or not necessarily lesser, in some cases)
Nonetheless, a noticeable group of such relatives are crushingly distressed by the whole deal, and campaign about it loudly in a way unusual for people who share the underlying neurotype
I think de novo mutations (including CNVs) explains some chunk of this. Definitionally, people whose diagnosable-autism or schizotypal-psychosis is intertwined with de novo mutations will have less schizotypal/autistic families than the general schizotypal/autistic population. They might also tend to have more dysfunctional presentations (this is clearly true of autism, the jury is out on psychosis), intensifying #3.
This is also presumably a factor in why some people are obsessed with implausible causes — vaccines, mercury, Torrey’s insistence you catch schizophrenia from viruses. People whose autistic or schizospec relatives are very unlike them are both more hostile towards said relatives and less able to make sense of a “these are archetypes of people and accordingly run in families” explanation. It’s very different to the “what do you mean this is weird, everyone in our family talks late/hears angels telling them what to do” cluster.
In practice, most support of the diametric model comes from Badcockian interpretations of it where schizotypy and autism are immediately-obvious opposites, which are not compatible with reality. They’re generally supported by autistic people who see it as in some way self-effacing, because that version of the hypothesis is fairly sympathetic towards a common autistic self-image (Badcock is clearly autistic). There is a sometimes-signalled, often-explicitly-stated reading of “well, that’s good, it says I’m the opposite of the real crazy people”. There’s a hell of a lot to say about that.
There's an issue here that people are simultaneously treating autism as a waste basket category (throwing anything that remotely looks like difficulties with socializing, sensory issues, etc) and wanting it to be a Real Thing. It can be one or the other, that's fine! We can decide that "autism" just refers to a list of symptoms that can be caused by any old thing--autism due to brain cancer. Autism due to being kicked by a mule. Autism due to anemia. Schizophrenia with autistic symptoms. OCD with autistic symptoms. Etc.--or we can decide that autism is a specific set of impairments with a particular cause, like Down's or the flu. What it CAN'T be is BOTH, and that's what trying to redefine WS as autism in order to save the autism/schiz dichotomy is trying to do.
People trying to better understand autism spectrum should be aware of this hypothesis which should be considered as a possible explanation for a subset of ASD.
(scroll to both places TripleTaco shows on the page)
https://slimemoldtimemold.com/2023/09/07/mysteries-contest-winners/
It presents a non-genetic cause which could explain the rise in diagnosis rates.